Health Conditions - Data
What you told us
- Patient Feedback for the Community Respiratory Team 2021 (PDF)
- Consultation and Engagement Report for Long Term Conditions for the Strategic Plan 2022-25 (PDF)
Impact Assessments
What the data tells us
Burden of Disease studies assess how ill-health and early death due to disease and injury prevent us from living longer and healthier lives. They use a single measure of health loss which combines the years lost to ill-health (years lived with disability) and the years lost due to early death (years of life lost). This measure is called the disability-adjusted life year (Public health Scotland, 2022).
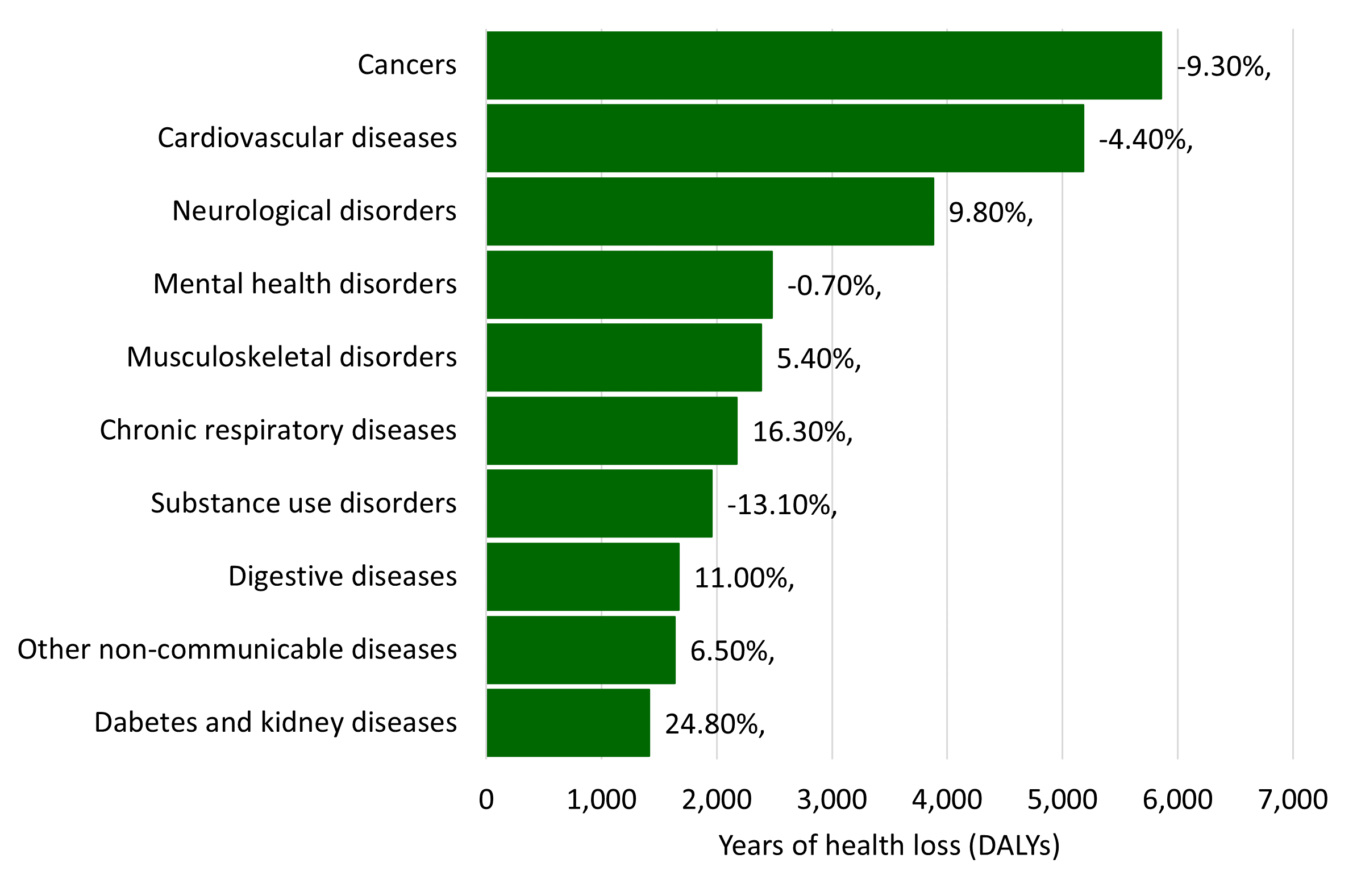
The three largest causes of ill-health and early death in Midlothian are cancers, cardiovascular diseases, and neurological disorders (Public Health Scotland, 2022). These account for 46% of the total burden of health loss. This is very similar to the rest of Scotland but there are some differences in Midlothian. The largest are due to diabetes and kidney diseases, chronic respiratory diseases and substance use disorders.
Leading grouped causes of ill health and early death
Data source: Public Health Scotland 2022
Health inequalities
Deaths in lower SIMD quintiles are more likely to be by avoidable deaths. The rate of health loss in the most deprived 5th of the population in the West region was 1.9 times higher than the rate in the least deprived 5th of the population. 47% of the health loss in the most deprived 5th of the population in the West region could have been avoided if the population in this quintile experienced the same rate as those in the least deprived 5th of the population (Public Health Scotland, 2022).
The leading causes of ill health and early deaths in the most deprived quintile are:
- Drug use disorders (9%),
- Ischaemic heart disease (7.5%)
- Lung cancer (6.5%).
The leading causes of ill health and early deaths in the least deprived quintile are:
- Alzheimer's disease and other dementias (7.4%),
- Ischaemic heart disease (7.2%)
- Low back and neck pain (5%).
Cancer
71.1% of people diagnosed with cancer survive for at least a year (Public Health Scotland, 2019).
Estimated one year survival decreased to 67.5% of people diagnosed with cancer (Public Health Scotland 2023).
Early detection: National screening programmes.
Bowel screening
- 67.9% people in Midlothian took up the offer of screening (2020-2022,a three-year rolling average uptake rate). This is an increase from 56.9% in 2015-2017. This is slightly higher than Scottish rates of 2020-2022 (66.2%) and 2015-2017 (56.5%) (Public Health Scotland)
- Screening uptake rates vary by inequality, with the gap between uptake rates in the most and least deprived at 20.1% (2023).
- Screening uptake rates vary by age, with 89% of over 75s taking up screening compared with 64% of 50–64-year-olds. Uptake rates increased across all ages groups (50 to 59, 60 to 74, and 75 and over) between 2018 and 2023.
Breast screening
- Screening uptake rates vary by inequality, with the gap between uptake rates in the most and least deprived at 16.1% (2023 Public Health Scotland)
Cervical screening
- 69.5% of people in Midlothian took up the offer of cervical cancer screening (2023/24)
- More women in the 50-64 age group were screened (71.4%) than the 25-59 age group (67.6%) (Public Health Scotland)
Diagnosed cancers
- 2,691 cancers (excluding non-melanoma skin cancer) were diagnosed in Midlothian (2015-2019).
- These were evenly split across genders, with 49% (1,352) of diagnoses in men and 51% (1,339) in women.
- Across the two localities, Midlothian (West) had more diagnoses of cancer with 54% of cases, compared to Midlothian (East) with 46%. (Macmillan Improving the Cancer Journey 2022).
62% of all cancer diagnosis in Midlothian are due to 6 types of cancer (for both males and females combined):
- Trachea, bronchus and lung cancer (Lung cancer has seen a downward trend in deaths with a wide range between East and West Midlothian).
- Female breast cancer (close to Scottish average)
- Colorectal cancer
- Prostate cancer
- Head and neck cancer
- Malignant melanoma of skin
Cancer registrations in Midlothian have risen since the mid-2010s, but have stabilised in the last few years. Three year averages of cancer diagnosis rates appear to be relatively stable in Midlothian between 2017 and 2022
- Locality - There appears to be no difference in diagnoses and whether you live in East or West Midlothian.
Increase in cancer rates
Given the number of people living with cancer in Midlothian in 2018 and Midlothian’s continued growing population, cancer rates are predicted to increase from 3,374 in 2018 to 4,237 in 2038.
Inequalities
Evidence from Public Health Scotland shows that socio-economic deprivation can influence cancer survival, people living in a more deprived area can be diagnosed at a later stage when survival is poorer. This is most evident in trachea, bronchus and lung cancer with 60% of lung diagnoses in SIMD quintiles 1 & 2. Others include 42% breast diagnoses and 40% of prostate diagnoses in SIMD quintiles 1 & 2.
Support for people affected by cancer
240 people in Midlothian were supported by 'Improving the Cancer Journey' (2023). The top 5 concerns of people were:
- money or finance,
- anxiety,
- fatigue,
- uncertainty
- thinking about the future.
Midlothian Macmillan Welfare Rights Partnership in 2022/2023 total financial gains for people with cancer were £526,772.73 plus an additional £6,880 Macmillan Grants totalling £533,652.73. A total number of 237 clients were assisted by the Welfare Rights Partnership, 95 of these clients were terminally ill which equates to 40% of the case load.
Respiratory Conditions
Respiratory conditions are those which affect the airways and other structures of the lung. Although 'respiratory condition' is a general term used to describe a large group of conditions, five conditions (Asthma, Bronchiectasis, Chronic Obstructive Pulmonary Disease, Idiopathic Pulmonary Fibrosis and Obstructive Sleep Apnoea Syndrome) make up 90% of the burden of respiratory disease in Scotland (Scottish Government, 2021.)
Asthma - a long-term lung condition which affects the airways and impacts breathing.
- 7.4 per 100 population in Midlothian have asthma (2025), which is comparable to the Scottish rate is 6.9 (Public Health Scotland, 2025).
Chronic Obstructive Pulmonary Disease (COPD) - progressive lung diseases including emphysema, chronic bronchitis, and refractory (non-reversible) asthma.
- 2.9 per 100 population in Midlothian have COPD (2025). This has increased from 2.7 per 100 population in 2022.
- More people are admitted to hospital with COPD in areas where people are more likely to experience disadvantage. The age-sex standardised rate of COPD hospitalisations is 122.4 per 100,000 population in Penicuik North and 257.2 per 100,000 population in Dalkeith (3-year aggregate figure 2021/22 to 2023/24) (ScotPHO Profiles, 2025). There were 162 potentially preventable admissions to hospital in 2024/25 for COPD (Discover, 2025).
Neurological Conditions
Neurological conditions, disorders and syndromes affect the brain, spinal cord, nerves and muscles. Examples include Multiple Sclerosis, Parkinson’s disease, Huntington’s disease, Motor Neurone Disease, epilepsy, seizures, chronic headache and migraine, acquired brain injury, dystonia, functional neurological symptoms, cerebral palsy and muscular dystrophy. Neurological conditions are the most common cause of serious disability in Scotland.
There is no reliable data on the number of people with a neurological condition and most services are co-ordinated at a Lothian level. A statistical estimate suggests there could be 5,300 people with a condition, 530 of whom will be disabled by the condition (Neurological Alliance, 2003). Neurological conditions account for between 10% and 20% of acute medical admissions in Scotland (Association of British Neurologists, 2017) and 10% of the overall burden of disease in Scotland, as measured by disability-adjusted life years (Scottish Public Health Observatory, 2017).
Multiple sclerosis
- An estimate of 188 people have multiple sclerosis in Midlothian (based on the prevalence rate in Scotland of 209 per 100,000, Multiple Sclerosis Trust, 2023).
- The proportion of women being diagnosed with multiple sclerosis is increasing - between two and three women have been diagnosed with multiple sclerosis for every man with the condition (Multiple Sclerosis Trust, 2023).
Parkinson’s disease
- An estimate of 240 people have Parkinson’s disease in Midlothian (based on the prevalence rate of 1 in every 375 adults in Scotland, Parkinson’s UK, 2023).
- People with Parkinson’s disease have a particularly high risk of hospital admission and are 6 times more likely to develop dementia as people of the same age without the condition (Parkinson’s UK, 2023).
- Nationally numbers are continuing to rise for both Multiple Sclerosis and Parkinson’s Disease. This is linked to people living longer with these conditions.
Huntington’s Disease
- An estimate of 14 people have Huntington’s Disease in Midlothian (based on the prevalence rate for Scotland of 16.1 people in every 100,000 from 1990-2010, Evans et al., 2013). (Scottish Huntington Association, 2023). The Scottish Huntington's Association reported a 55% increase in diagnoses between 2012 and 2015.
Motor Neurone Disease (MND)
- Current estimates of MND prevalence in Scotland suggest between 300-450 people living with MND in Scotland at any given time (5.5 to 7.4 per 100,000) (ScotPHO, 2016). The median survival time for motor neurone disease in Scotland is 25 months (ScotPHO, 2016).
Stroke
A stroke occurs when the blood supply to part of the brain is compromised, often by a blood clot blocking an artery or a ruptured blood vessel. The effects of a stroke may alter someone's ability to move, feel, think, communicate, and function.
- 1,943 people in Midlothian have had a stroke (based on the prevalence rate in Midlothian (the number of people registered at one particular point in time) for stroke/TIA of 2.42 per 100 patients, Public Health Scotland 2022). This is above the Scottish average prevalence rate (2.21) (Public Health Scotland 2022).
- Nationally the death rate for cerebrovascular disease in the most deprived areas was 46% higher than in the least deprived areas in 2019 (Public Health Scotland 2023).
- 74% of people were discharged to their own homes after admission to hospital for a stroke/TIA
- 16% of people were discharged to a care home after admission to hospital for a stroke/TIA.
- 50% of people were discharged within 3 days or less (April 19-Aug 20) (VOCAL, 2017)
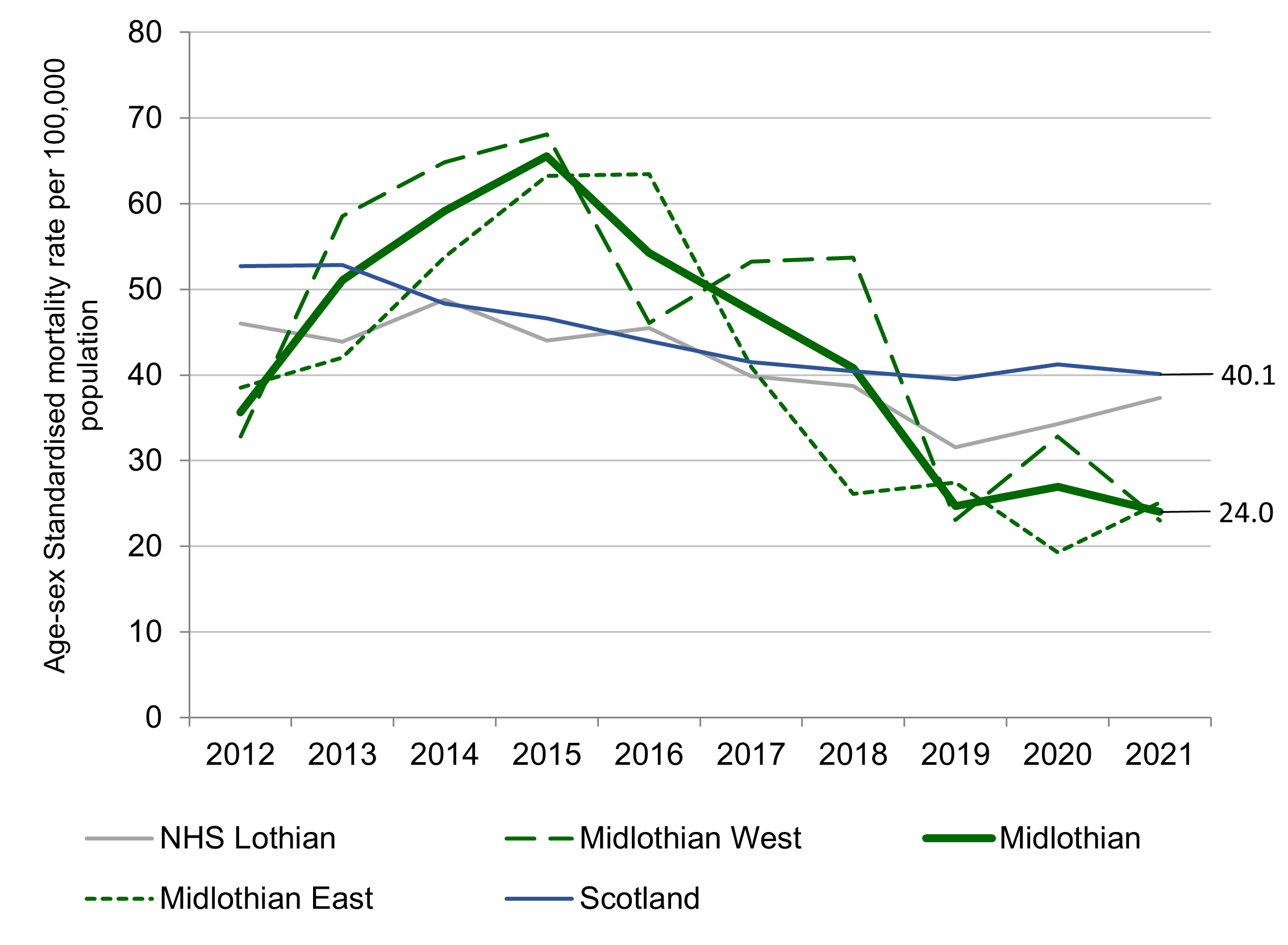
All Age Stroke Mortality, Midlothian Locality, NHS Lothian and Scotland
Data source: Public Health Scotland.
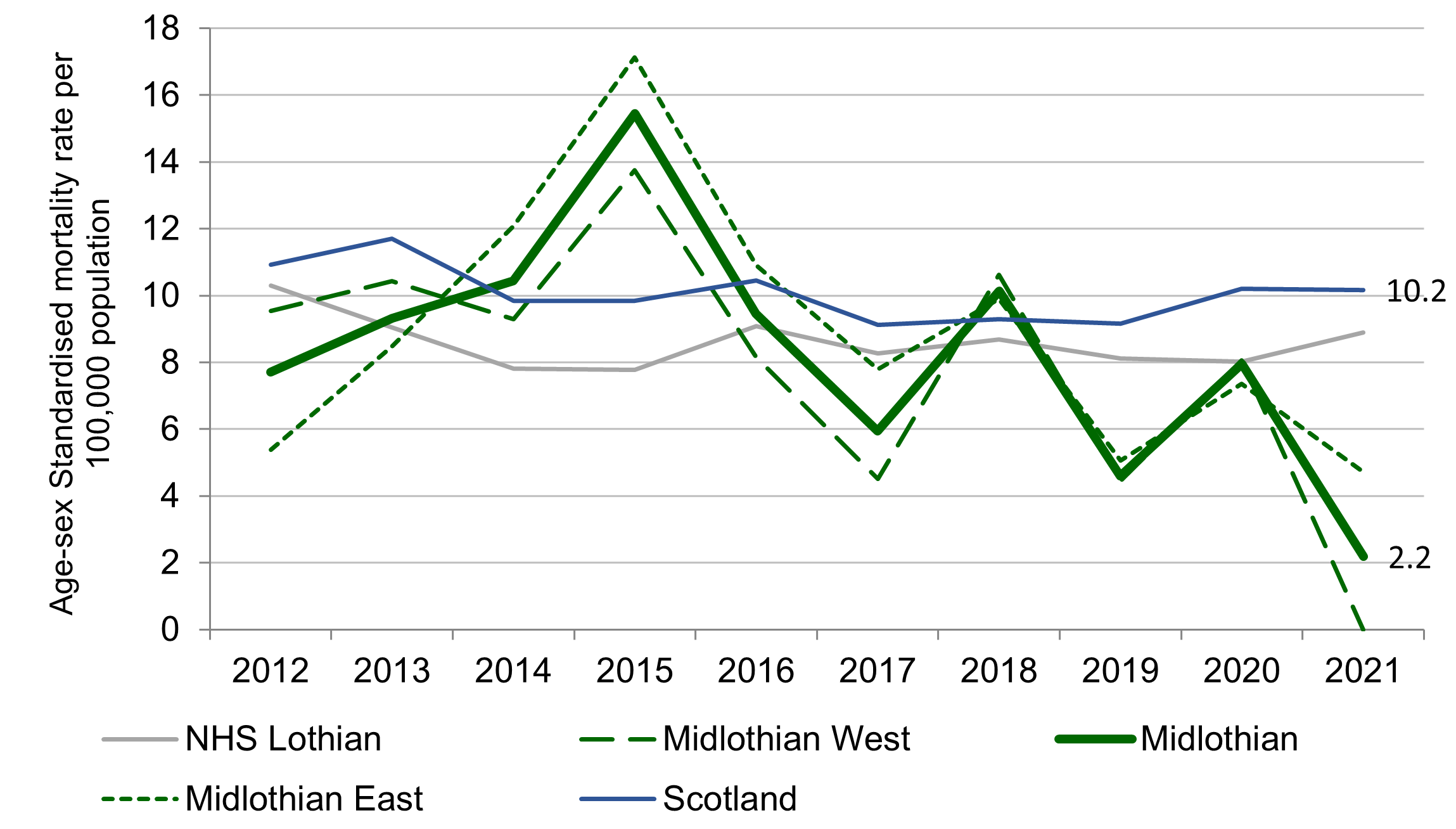
Early (<75) Stroke Mortality, Midlothian Locality, NHS Lothian and Scotland
Data source: Public Health Scotland
Diabetes
Over 317,000 people have a diagnosis of diabetes in Scotland in 2020 (Scottish Diabetes Survey), a crude prevalence of 5.8% (compared to 5.1% in 2013). This represents an increase of over 4,700 people since 2019.
- Type 1 diabetes often starts at a young age and is due to a lack of insulin. It accounts for 10.7% of cases in Scotland (2020 ScotPHO).
- Type 2 diabetes starts with resistance to the action of insulin and is associated with older age, being overweight and obesity (ScotPHO, 2022).
Approximately 80% of diabetes complications are preventable or can be delayed through early detection, good care and access to appropriate self-management tools and resources. In England, obese adults are five times more likely to be diagnosed with diabetes than adults of a healthy weight (Public Health England, 2014).
Diabetes care accounts for around 10% of all NHS expenditure. If no changes are made to the way diabetes is treated by 2035 ⁄ 2036, it is estimated that this will rise to around 17% of NHS expenditure (Hex et al., 2012).
Number of people in Midlothian with Diabetes
- Sex - there was a higher proportion of males (55.95%) than females (44.05%) with type 2 diabetes between 2015/16 and 2020/21.
- Age - Type 2 diabetes is most prevalent in older people but increasing numbers of younger people are being diagnosed.
Inequalities
The group with the highest rate (per 100,000) of diagnosis are those in SIMD 5 (2015/16 - 2022/23)
- SIMD 1 - 214
- SIMD 2 - 898
- SIMD 3 - 599
- SIMD 4 - 410
- SIMD 5 - 259
Page updated: March 2026